 Leonie L. Rübig1,2Jürgen Fuchshuber2,3Pia Köldorfer2Anita Rinner2
Leonie L. Rübig1,2Jürgen Fuchshuber2,3Pia Köldorfer2Anita Rinner2 Andreas Fink2
Andreas Fink2 Human-Friedrich Unterrainer2,4,5*
Human-Friedrich Unterrainer2,4,5*- 1Institute of Psychology, University of Graz, Graz, Austria
- 2CIAR: Center for Integrative Addiction Research, Grüner Kreis Society, Vienna, Austria
- 3Department of Philosophy, University of Vienna, Vienna, Austria
- 4Department of Psychiatry and Psychotherapeutic Medicine, Medical University Graz, Graz, Austria
- 5Department of Religious Studies, University of Vienna, Vienna, Austria
Background: There is convincing evidence that individuals suffering from Substance Use Disorder (SUD) often present insecure attachment patterns. In contrast, a strong therapeutic alliance in treatment of SUD has been found to lead to a more positive treatment outcome. However, insecure attachment has been observed to be linked with weaker therapeutic alliance strength. The primary aim of this explorative study was to gain initial insights regarding the influence of attachment and personality characteristics on therapeutic alliance and therapy motivation in SUD patients undergoing treatment at a therapeutic community. Furthermore, SUD patients were compared to healthy controls regarding attachment, personality and mood pathology.
Methods: A total sample of 68 participants, 34 inpatients in SUD treatment and 34 age-gender and education adjusted controls, were investigated. Both groups filled in the Adult Attachment Scale (AAS), the Inventory of Personality Organization (IPO-16), and the Brief Symptom Inventory (BSI-18) questionnaires. Additionally, SUD patients filled in the Working Alliance Inventory (WAI-SR) and the adapted German version of the University of Rhode Island Change Assessment scale (FEVER).
Results: In line with our assumptions, SUD patients exhibited a decreased amount of attachment security (AAS) which was related to higher personality (IPO-16) and mood pathology (BSI-18). Furthermore, correlational analysis revealed the WAI-SR dimension Bond being positively associated with more secure attachment. A strong task alliance was linked to the Action stage of change (FEVER) and decreased mood but not personality pathology.
Conclusion: Our findings confirm the putative negative effect of attachment and personality pathology on therapy motivation and therapeutic alliance in addiction therapy as well as more specifically in therapeutic community treatment. Future research in enhanced samples might focus more on the long-term effects of the interaction of attachment, personality and therapeutic alliance variables.
Introduction
In 2019, nearly 26,000 people in Austria suffering from Substance Use Disorder (SUD) were in long-term outpatient or inpatient drug-specific treatment. Additionally, there is a highly problematic rate of dropouts around 54% in inpatient drug treatment (1). In contrast, drug treatment retention in terms of the length of stay has been shown to be one of the most important predictors of favorable follow-up treatment outcomes (2, 3). Therefore, keeping patients in treatment is one of the main objectives in SUD therapy and correspondingly, the philosophy of drug-free therapeutic communities is to establish sustainable relationships by building on self-help and mutual-aid between patients. Hereby, the community acts as the central attachment figure, as most of the therapy takes place in group dynamic processes between the clients. Therapists mostly just monitor group dynamics and are mainly responsible for single-therapy sessions (4).
Across various psychotherapeutic approaches, therapeutic alliance is one of the most widely studied process variables in psychotherapy research, mainly because of its obvious link to a positive or negative therapy outcome (5, 6). The concept of therapeutic alliance originates from traditional psychoanalysis and was conceptualized as being closely related to the mechanisms of transference (7). However, early approaches considered therapeutic alliance more as a bonding concept, while Bordin (8) later conceptualized it as a working relationship between client and therapist, emphasizing its cooperative nature (6). Following Bordin's model of alliance as working alliance), it is composed of the three dimensions bond, goals, and tasks, i.e., an affective relationship component, the jointly determined therapy goals, and the process-related tasks of therapist and client (8).
Numerous empirical studies emphasize the substantial relationship between therapeutic alliance and positive treatment outcomes, independent of potential confounders such as cultural background, therapist profile, type of treatment or research design (9–11). This is consistent with the findings from therapy outcome research focusing on SUD treatments (12, 13). Nevertheless, recent studies suggest the relationship between therapeutic alliance and positive outcomes to be lower in SUD patients, by reporting weak correlations of around r = 0.14 (9, 14). What is more, various client characteristics have been observed to play an important role for the relationship between therapeutic alliance and the course of SUD treatment. Based on an enhanced literature review, Meier et al. (13, 15) argue that neither SUD patients' demographic nor diagnostic pre-treatment characteristics predicted good therapeutic alliance. However, they found a significant number of studies showing modest relationships for positive previous treatment experience, motivation and treatment readiness, coping strategies, social support and secure attachment.
Attachment pathology has received an increased interest as a potential vulnerability factor in the context of SUD, as insecure attachment patterns can be frequently observed in SUD patients (16–18). In correspondence to this, SUD has been regarded as a certain kind of attachment disorder (19), see also (20) for an enhanced review). Experiences with insufficient attachment figures (in most cases the parents) cause severe emotional disturbances within the child and lead to the formation of deficient internal working models in relation to the self and other people later in life (16, 21–23). Correspondingly, substance use can be described as a kind of “self-medication” in order to regulate affects by means of chemical substances (23, 24). Therefore, from the perspective of attachment theory, therapeutic communities try to break this bond to a harmful substance use or activity and aims to replace it by a bond to the community, with the therapeutic community acting as an attachment figure (19, 25, 26).
Despite of conflicting results [e.g., (26)] attachment organization might have a huge impact regarding an increased alliance, as securely attached individuals were observed to exhibit stronger alliance values than insecurely attached ones (27–30). Correspondingly, Gidhagen et al. (14) reported attachment styles as to be a significant moderator variable between higher working alliance and positive therapy outcome in a sample of SUD patients. Furthermore, there is significant evidence for the substantial connection of attachment organization and personality structure (31). In general, SUDs are often seen as co-occurring with a dysfunctional personality structure as 34–73% of SUD patients were diagnosed for comorbid personality disorder, despite the fact that there is only a prevalence rate of about 10% for the presence of personality disorder in the general population (32–34). What is more, borderline personality organization seems to be associated in particular with the development of SUD (35, 36). In terms of therapy outcome, the occurrence of personality disorders has been shown to be linked to negative treatment outcome like early treatment dropout (12, 37). On the other hand, a strong alliance turned out to be a substantial positive predictor of treatment success (38). However, as personality disorders often cause problematic interpersonal relationships, they can impede the formation of an alliance (39, 40).
Therapy motivation has been reported as a highly important variable as no or low therapy motivation is one of the major challenging problems in the treatment of SUD, throughout the entire therapeutic process. This applies to different phases of therapy as well as to maintaining therapy goals and avoiding relapse. Frequently, treatment is only sought when the physical condition becomes so severely damaged that external help is inevitable, or social pressure becomes too strong. In many cases, inconsistency between actual behavior and a supposedly high verbally communicated therapy motivation can be observed. Once acute problems have subsided, therapy is often terminated prematurely (41).
The transtheoretical model of DiClemente and Prochaska (42) assumes five stages of change in human behavior, each describing the motivational state of the person, as well as the motivation for change (43). As to positive outcomes, low treatment readiness leads to e.g., short-term retention and SUD clients in the pre-contemplation stage are more likely to drop out of therapy prematurely, while clients in the action stage are more likely to actively engage in self-change (43–45). Most importantly, growing evidence has been supporting the idea of readiness for change and certain stages to predict alliance strength (13, 45–47). Ilgen et al. (48) found a positive and strong alliance to be especially important for patients with low therapy motivation, highlighting the potentially beneficial relation between higher stages of change and working alliance. Finally, the putative link regarding SUD and mood pathology has already been extensively investigated in the past and there is evidence that a positive therapeutic alliance might be especially important in keeping SUD clients with additional psychiatric comorbidity in treatment [e.g., (13, 49, 50)].
Research Aims
Primarily, this study aims to explore the potential link between different attachment dimensions and therapeutic alliance/ therapy motivation in SUD patients undergoing treatment within the surroundings of the therapeutic community. Furthermore, it is intended to compare SUD patients to healthy controls in terms of several parameters of attachment and personality pathology to further examine the assumption of substance misuse as a dysfunctional way of emotion regulation. In line with the primary hypothesis of this study, this investigation might further elucidate the specific challenges regarding the treatment of addiction disorders.
Method
Participants and Procedure
A total sample of 68 male (86.8%) and female (13.2%) participants between 20 and 61 years of age (M = 33.3, SD = 9.7), consisting of one clinical (n = 34) and one non-clinical control group (n = 34), was investigated. Samples were adjusted in terms of Age, Gender and Education status. All participants of the clinical group were diagnosed for SUD according to the International Classification of Diseases version 10 (ICD 10) (51), by a licensed psychiatrist. These patients were undergoing inpatient therapy in the drug-free environment of an Austrian TC, hosted by the Grüner Kreis society, at the time of the study. In terms of the consumed psychoactive substances the following percentages could be observed: 29.1% Opioids (ICD-Code: F11), 19.0% Alcohol (F10), 19.0% Cannabinoids (F12), 13.9% Sedatives or hypnotics (F13), 11.4% Cocaine (F14) and 7.6% Other stimulants (F15). 76.5% of patients reported poly drug use. Comorbidities with other diagnosis were distributed as follows: 21.4% Affective disorders (F3.x), 16.7% Neurotic, stress-related and somatoform disorders (F4.x), 7.1% Personality and behavioral disorders (F6.x), 7.1% Schizophrenia, schizotypal and delusional disorders (F2.x) and 2.4% Behavioral and emotional disorders with onset usually occurring in childhood and adolescence (F5.x). The sample for the control group was taken from the normal population by means of an internet survey, distributed through social networks. Hereby, the inclusion criterion was an Age range from 18 to 65 years. Exclusion criteria were a diagnosis of SUD and/or any kind of diagnosed mental disorder, either at the time of the study or in the past. Nicotine dependence was not considered in this study. The study protocol was approved by the ethics committee of the University of Graz, Austria. Data of the clinical sample were acquired in a one-time group testing in the therapeutic community in July 2020. Data of the non-clinical sample were collected via the online-survey platform LimeSurvey© in November 2020. Written informed consent was given by all participants before answering the questions.
Psychometric Instruments
Mood Pathology
The short version of the Brief Symptom Inventory [BSI-18; (52); German version: (53)] assesses psychological distress within the past seven days. The inventory includes three subscales: (1) Somatization, (2) Depressiveness and (3) Anxiety. It consists of 18 items in total, which are rated on a 5-point Likert scale ranging from not at all (0) to very much (4). By summing up all the three scale scores, a Global Severity Index (GSI) can be generated that provides information about the overall severity of general psychiatric symptoms. Cronbach's α in this study ranged from 0.75 to 0.84. for the subscales. The total GSI score showed a Cronbach's α of 0.91.
Attachment Styles
The German Version of the Adult Attachment Scale [AAS; (54, 55)] is a self-descriptive measure of attachment-related attitudes consisting of 15 items answered on a 5-point Likert scale, ranging from strongly disagree (1) to strongly agree (5). The questionnaire is based on Bowlby's attachment theory (56) and consists of three subscales: (1) Anxiety about being rejected or unloved (“Anxiety”), (2) Comfort with closeness and intimacy (“Closeness”) and (3) Comfort in depending on others (“Dependence”). Cronbach's α for the scales ranged from 0.76 to 0.86.
Personality Organization
The Inventory of Personality Organization—Short Version [IPO-16; (57)] is a self-report instrument to assess personality organization according to Otto Kernberg's model (58). The IPO-16 is composed of 16 items, which are rated on a 5-point Likert scale ranging from never true (1) to always true (5). The total score is a global measure representing the extent of structural deficit and can serve as an indicator of the presence of a personality disorder. In this study we observed good internal consistency for the scale with a Cronbach's α of 0.88.
Readiness to Change
The “Fragebogen zur Erfassung der Veränderungsbereitschaft” questionnaire [FEVER; (59)] is the German version of the University of Rhode Island Change Assessment Scale [URICA; (60)] based on the transtheoretical model of change by DiClemente and Prochaska (42). The FEVER is a self-descriptive procedure to measure readiness to change and to assess therapy motivation in complex problem behaviors. Instead of pointing a person into one single stage, the FEVER provides scores for each of the three temporal-motivational dimensions corresponding to the stages of change: Precontemplation, Contemplation, and Action. The 24 items can be answered on a 5-point Likert scale from not true at all (1) to very true (5). Cronbach's α for the three scales ranged from 0.80 to 0.84.
Therapeutic Alliance
The German client version of the Working Alliance Inventory—short revised [WAI-SR; (61)] is based on the frequently used Working Alliance Inventory (WAI) by Horvath and Greenberg (62). The WAI is theoretically based on Bordin's (8) conception of the therapeutic alliance and therefore measures the three working alliance dimensions of Bond, Tasks and Goals. The 12 items of the WAI-SR are rated using a 5-point Likert scale ranging from rarely (1) to always (5). Participants were asked to rate the relationship to their reference therapist. Internal consistency was acceptable to good with Cronbach's α ranging from 0.77 to 0.87.
Data Analysis
SPSS 26 was used for statistical analyses. For group comparisons, one-way or multivariate analyses of variance and χ2 tests were conducted. To investigate the relationship between behavioral measures and the three dimensions of working alliance in the clinical group, Pearson's correlation coefficients were calculated. As the requirement of normal distribution for the use of parametric statistical methods was violated for some variables, equivalent non-parametric procedures were conducted in these cases. Furthermore, in cases where linearity assumption was not given, non-parametric Spearman rank-correlation was also calculated. However, these proceedings did not lead to any deviating result. In order to control for α-inflation, the level of significance was set to p < 0.01 in ANOVAs, and Pearson's and Spearman's correlations, while p-values < 0.05 were marked as tendencies, but where not further interpreted. Where it was feasible, effect sizes were included.
Results
Demographics and Sample Characteristics
Socio-demographic variables of both groups as well as resulting group differences are presented in Table 1.
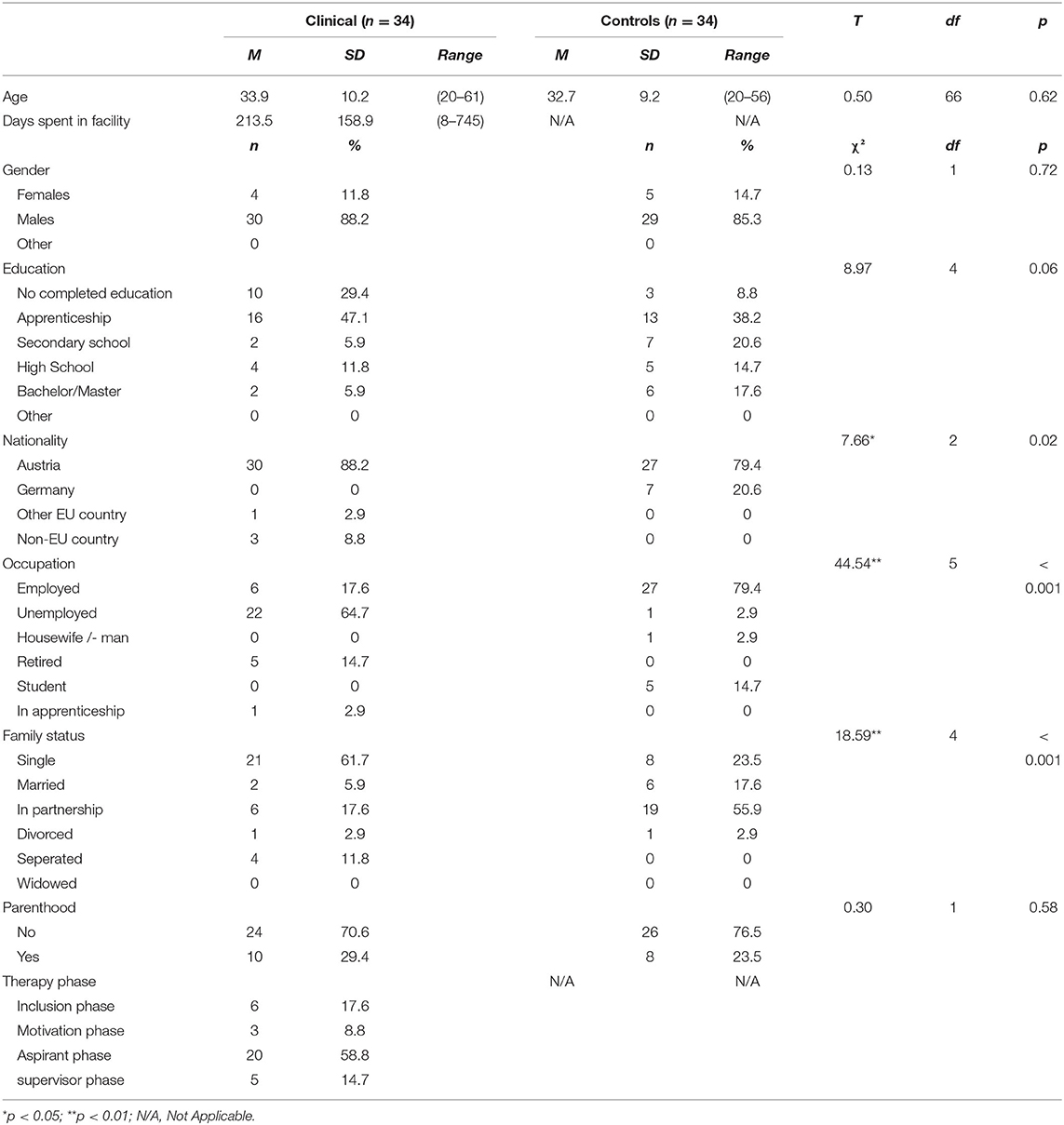
Table 1. Sociodemographic data with group differences.
Group Differences in Behavioral Measures
As shown in Table 2, group comparisons between the clinical and the control group showed that the clinical SUD sample reported significantly higher values on all behavioral dimensions than non-clinical controls did. In correspondence to this, SUD patients exhibited more severe deficits in personality organization, higher mood pathology and less secure attachment attitudes (F = 8.99–68.02; η2 = 0.12–0.50; all p < 0.01).
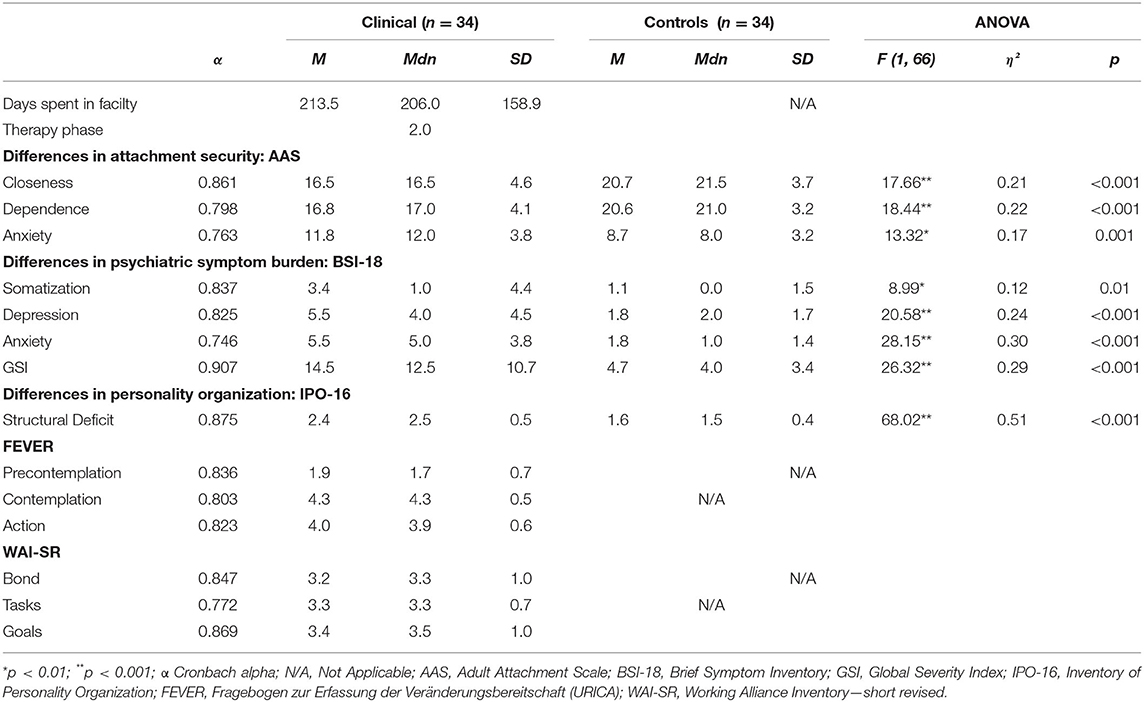
Table 2. Group differences in behavioral measures.
Correlations Between Behavioral Measures and Working Alliance Dimensions in SUD Patients
As demonstrated in Table 3, we observed the “Bond” dimension of working alliance to be strongly positively associated with the attachment dimension “Dependence” (r = 0.61; p < 0.001). Furthermore, the “Tasks” dimension was negatively related to BSI subscale “Anxiety” (r = −0.44; p < 0.01) and the overall BSI total score “GSI” (r = −0.44; p < 0.01), as well as “Action” stage of change (r = 0.45; p < 0.01). No significant relations were found between the “Goals” dimension and any of the examined variables (p > 0.01) apart from intercorrelating working alliance dimensions (p < 0.01). Also, no significant relations were found between the IPO “Structural deficit” total score and working alliance (p > 0.01). The attachment dimension “Dependence” and “Structural deficit” correlated negatively (r = −0.47, p < 0.01), while “Anxiety” about being rejected or unloved and “Structural deficit” correlated positively (r = 0.59; p < 0.001). Finally, we observed a positive association between the “Precontemplation” stage and “Structural deficit” (r = 0.47; p < 0.01). Overall, all significant correlations were moderate to strong. No significant correlations were observed regarding age and sex (all p > 0.05).
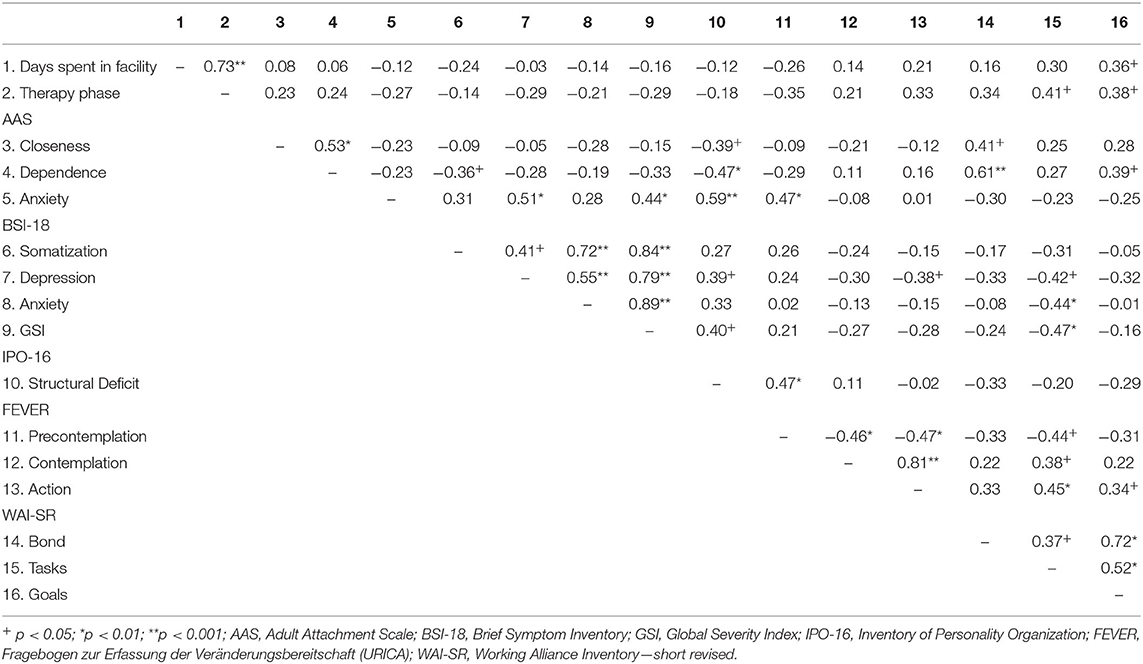
Table 3. Intercorrelations for behavioral measures within the SUD sample (n = 34).
Discussion
In this study it was primarily aimed to explore the putative link between attachment and personality characteristics and task alliance, namely the three dimensions of working alliance “Bond,” “Tasks,” and “Goals,” in SUD patients undergoing treatment within the surroundings of a therapeutic community. In line with our assumptions, attachment security showed a strong positive correlation with the “Bond” dimension. Accordingly, the “Bond” dimension in particular refers to the personal bonding experience between therapist and client. This experience is built on more affective aspects of the therapeutic relationship like confidence, acceptance or mutual trust (7). Moreover, this finding is confirmed by previous research [e.g., (27, 28)].
Furthermore, in order to shed further light on the question why substance use disorders are assumed to be notoriously difficult to treat (1), we investigated possible differences regarding attachment and personality between healthy controls and patients diagnosed with SUD. In correspondence to this, we found SUD patients to differ significantly from an age-gender and education adjusted control group by exhibiting diminished attachment security, as well as higher amounts of personality and mood pathology. These findings are highly consistent with the literature [e.g., (16, 17, 34, 35, 49, 63)].
In addition, resonating with previous studies, we found an increased personality structural deficit to be related to more insecure attachment [e.g., (31)]. More in general, these findings further underline the well-established assumption of substance misuse as a dysfunctional way of emotion regulation (63, 64). Taken together, these results seem to suggest that one of the difficulties in the treatment of SUD might be related to addiction specific problems regarding attachment security. However, further research needs to be done, comparing different patient populations (e.g. SUD patients vs. mood disorder patients) to further investigate this assumption.
Moreover, we explored correlation patterns of attachment and personality dysfunctioning, mood pathology, and therapy motivation readiness in SUD patients. As to mood pathology, clients who felt less anxious and demonstrated a less severe overall mood pathology rated the “Tasks” working alliance with their therapist to be moderately stronger. We only found clients in the “Action” stage of treatment readiness to exhibit a higher “Tasks” working alliance with their therapists. This relates to findings of Fitzpatrick and Irannejad (65) who found higher stages of change in adolescents being strongly related to higher “Tasks” and “Goals” working alliance, highlighting their collaborative nature. More in general, our results support the idea of a potentially beneficial relation between higher stage of change and working alliance. Interestingly, mood disorder related symptoms like anxiety often affect motivation and clients in a higher stage of change have been observed to exhibit stronger working alliance and symptom improvement (46, 47). In contrast, we observed that clients in “Precontemplation” stage exhibited a more severely impaired personality structure and described themselves as feeling more anxious about being rejected or unloved. This aspect of insecure attachment was also related to an increased mood pathology. The findings suggest that less pathology in patients is associated with higher treatment readiness. Consequently, they could have been more capable to engage in a strong working alliance. On the other hand, a weak working alliance would likely not have contributed to symptom improvement. Therefore, our results might reflect these connections. Against our expectations, personality pathology was not significantly correlated to working alliance dimensions. This finding is in contrast to previous results, where higher levels of impaired personality organization impeded working alliance formations in residential treatment of SUD (40).
Our study offers additional insights into the putative effect of attachment and personality pathology on working alliance and therapy motivation in SUD patients, by expanding these findings for the therapeutic community environment. In this study we focused on the examination of alliances between SUD clients, but further research is needed to investigate within-patient therapeutic alliance. This might contribute to more knowledge regarding the specific direction of the association between therapeutic alliance and symptomatic improvement, as previously pointed out by Gidhagen et al. (14). Does a stronger therapeutic alliance lead to symptomatic improvement or does the decrease of symptoms increase therapeutic alliance? Current studies mostly find therapeutic alliance to predict symptom improvement, but an interplay is also very likely, especially regarding common therapeutic alliance fluctuation and ruptures throughout treatment (7, 11, 66).
Limitations and Future Perspectives
Due to the exploratory nature of this study, its main limitation is the small number of participants. Moreover, since inconsistent therapeutic alliance developments have been observed, a longitudinal study approach applying therapeutic alliance oriented measures might probably deliver in-depth insights into its development over time, providing a trait-like characteristic instead of state-alliance (5, 7). Additionally, only self-report measures were used in this study. As to therapeutic alliance measures, previous research found client-rated therapeutic alliance to be most predictive for outcome variables like dropout [e.g., (67)]. However, in fact therapists' assessment of therapeutic alliance has sometimes been found to be a more precise predictor [e.g., (68)]. Therefore, it would be appealing for future research to investigate possible deviations in client and therapist perception of their therapeutic alliance. Likewise, this study did not investigate the impact of same-gender or different-gender therapist/patient pairings, which might have had an influence on therapeutic alliance. Hence, further studies should consider the patient-therapist gender match as a potential confounding variable. Another limitation of this study is that neither severity nor duration of the SUD diagnoses were assessed in our patient sample. It is also important to state that individuals suffering from SUD form a quite heterogenous group often presenting a variety of comorbid psychiatric disorders (50). This circumstance might also have affected our findings. A study with larger samples would make it possible to differentiate between specific SUD diagnoses. Similarly, due to the small sample size of controls diagnosed with mood disorders, we were unable to include these participants as a separate group. Hence, to avoid a possible confounding variable in our control group we decided to exclude these participants. Nevertheless, comparisons of participants with mood disorders and patients suffering from SUD might be a particularly interesting research topic, as mood disorders pose a significant vulnerability to develop addictions (64).
Finally, literature suggests the associations between therapeutic alliance and attachment to be more complex with various intervariable connections [e.g., (14, 27)]. In order to gain an enhanced understanding of the relationship between working alliance dimensions and attachment, as well as personality, mood pathology and therapy motivation, future research might focus on more complex research designs in SUD samples. Also, it would be feasible to include therapy outcome as a dependent variable and to examine possible mediational relationships regarding attachment, personality organization and therapeutic alliance. In correspondence to this, other variables that have been observed to play a role in the attachment-alliance linkage—such as the type of experienced abuse—should be considered in future studies [e.g., (14)].
Conclusion
Still, some notable implications for treatment of SUD can be derived from our findings: They highlight once more the importance of therapeutic alliance as a beneficial relationship between client and therapist in SUD treatment. However, regarding the diminished attachment security often found in SUD patients, this might be an especially challenging task for practicians working with this patient population. In conclusion, our findings point toward the need to take the client's attachment style into account while establishing the therapeutic alliance and to carefully consider related pathologies and motivational aspects.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by University of Graz. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
LR, AF, and H-FU conceptualized the study. LR, AR, and PK collected the data. LR and JF analyzed and interpreted the data. LR and H-FU drafted the manuscript. JF, AR, PK, AF, and H-FU critically reviewed it. All authors gave their final approval of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Anzenberger J, Busch M, Gaiswinkler S, Grabenhofer-Eggerth A, Klein C, Schmutterer I, et al. Epidemiologiebericht SUCHT 2020: Illegale Drogen, Alkohol und Tabak. Wien: Gesundheit Österreich. (2020).
2. Hubbard RL, Craddock SG, Anderson J. Overview of 5-year followup outcomes in the drug abuse treatment outcome studies (DATOS). J Substan Abuse Treat. (2003) 25:125–134. doi: 10.1016/S0740-5472(03)00130-2
3. Simpson DD. A conceptual framework for drug treatment process and outcomes. J Subst Abuse Treat. (2004) 27:99–121. doi: 10.1016/j.jsat.2004.06.001
4. De Leon G. The Therapeutic Community: Theory, Model, and Method. New York, NY: Springer Publishing Company. (2000).
5. Flückiger C, Horvath A, Del Re AC, Symonds D, Holzer C. Die Bedeutung der Arbeitsallianz in der Psychotherapie. Psychotherapeut. (2015) 60:195–8. doi: 10.1007/s00278-015-0020-0
6. Hentschel U. Therapeutic alliance: Part 2: Further considerations on the relationship and discernability of the concept to similar constructs. Psychotherapeut. (2005) 50:385–93. doi: 10.1007/s00278-005-0446-x
7. Horvath AO, Luborsky L. The role of the therapeutic alliance in psychotherapy. J Consult Clin Psychol. (1993) 61:561–73. doi: 10.1037/0022-006X.61.4.561
8. Bordin ES. The generalizability of the psychoanalytic concept of the working alliance. Psychotherap Theory Res Pract. (1979) 16:252–60. doi: 10.1037/h0085885
9. Flückiger C. The alliance in adult psychotherapy: a meta-analytic synthesis. Psychotherap Theory Res Pract Train. (2018) 55:316–40. doi: 10.1037/pst0000172
10. Horvath AO, Del Re AC, Flückiger C, Symonds D. Alliance in individual psychotherapy. Psychotherapy. (2011) 48:9–16. doi: 10.1037/a0022186
11. Zilcha-Mano S, Errázuriz P. One size does not fit all: examining heterogeneity and identifying moderators of the alliance-outcome association. J Couns Psychol. (2015) 62:579–91. doi: 10.1037/cou0000103
12. Brorson HH, Ajo Arnevik E, Rand-Hendriksen K, Duckert F. Drop-out from addiction treatment: a systematic review of risk factors. Clin Psychol Rev. (2013) 33:1010–24. doi: 10.1016/j.cpr.2013.07.007
13. Meier PS, Barrowclough C, Donmall MC. The role of the therapeutic alliance in the treatment of substance misuse: A critical review of the literature. Addiction. (2005) 100:304–16. doi: 10.1111/j.1360-0443.2004.00935.x
14. Gidhagen Y, Holmqvist R, Philips B, Falkenström F. The role of the working alliance in psychological treatment of substance use disorder outpatients. Psychother Res. (2020) 31:551–72. doi: 10.1080/10503307.2020.1807639
15. Meier PS, Donmall MC, Barrowclough C, McElduff P, Heller RF. Predicting the early therapeutic alliance in the treatment of drug misuse. Addiction. (2005) 100:500–11. doi: 10.1111/j.1360-0443.2005.01031.x
16. Schindler A. Attachment and substance use disorders: theoretical models, empirical evidence, and implications for treatment. Front Psychiatry. (2019) 10:727. doi: 10.3389/fpsyt.2019.00727
17. Unterrainer HF, Hiebler-Ragger M, Koschutnig K, Fuchshuber J, Tscheschner S, Url M, et al. Addiction as an attachment disorder: white matter impairment is linked to increased negative affective states in poly-drug use. Front Hum Neurosci. (2017) 11:208. doi: 10.3389/fnhum.2017.00208
18. Unterrainer HF, Hiebler-Ragger M, Rogen L, Kapfhammer HP. Sucht als Bindungsstörung. Nervenarzt. (2018) 89:1043–8. doi: 10.1007/s00115-017-0462-4
19. Flores PJ. Addiction as an attachment disorder: implications for group therapy. Int J Group Psychother. (2001) 51:63–81. doi: 10.1521/ijgp.51.1.63.49730
20. Hiebler-Ragger M, Unterrainer HF. The role of attachment in poly-drug use disorder: an overview of the literature, recent findings and clinical implications. Front Psychiatry. (2019) 10:579. doi: 10.3389/fpsyt.2019.00579
22. Fonagy P, Gergely G, Target M. The parent–infant dyad and the construction of the subjective self. J Child Psychol Psychiatr. (2007) 48:288–328. doi: 10.1111/j.1469-7610.2007.01727.x
23. Schindler A. “Bindung und Sucht: Theoretische Modelle, empirische Zusammenhänge und therapeutische Implikationen,” In: Brisch K, editor. Bindung und Sucht. Stuttgart: Klett-Cotta (2013). p. 13–31.
24. Khantzian EJ. Self-regulation and self-medication factors in alcoholism and the addictions: similarities and differences. Nat Counc Alcohol. (1990) 8:255–71.
25. De Leon G, Unterrainer HF. The therapeutic community: a unique social psychological approach to the treatment of addictions and related disorders. Front Psychiatry. (2020) 11:786. doi: 10.3389/fpsyt.2020.00786
26. Fuchshuber J, Hiebler-Ragger M, Ragger K, Rinner A, Kapfhammer HP, Unterrainer HF. Increased attachment security is related to early therapy drop-out in substance use disorders. BMC Res Notes. (2018) 11:141. doi: 10.1186/s13104-018-3251-7
27. Bachelor A, Meunier G, Laverdiére O, Gamache D. Client attachment to therapist: relation to client personality and symptomatology, and their contributions to the therapeutic alliance. Psychotherap Theory Res Pract Train. (2010) 47:454–68. doi: 10.1037/a0022079
28. Byrd KR, Patterson CL, Turchik JA. Working alliance as a mediator of client attachment dimensions and psychotherapy outcome. Psychotherapy Theory Res Pract Train. (2010) 47:631–6. doi: 10.1037/a0022080
29. Diener MJ, Monroe JM. The relationship between adult attachment style and therapeutic alliance in individual psychotherapy: a meta-analytic review. Psychotherapy. (2011) 48:237–48. doi: 10.1037/a0022425
30. Smith AEM, Msetfi RM, Golding L. Client self rated adult attachment patterns and the therapeutic alliance: a systematic review. Clin Psychol Rev. (2010) 30:326–37. doi: 10.1016/j.cpr.2009.12.007
31. Fuchshuber J, Hiebler-Ragger M, Kresse A, Kapfhammer HP, Unterrainer HF. The influence of attachment styles and personality organization on emotional functioning after childhood trauma. Front Psychiatry. (2019) 10:643. doi: 10.3389/fpsyt.2019.00643
32. Bowden-Jones O, Iqbal MZ, Tyrer P, Seivewright N, Cooper S, Judd A, et al. Prevalence of personality disorder in alcohol and drug services and associated comorbidity. Addiction. (2004) 99:1306–14. doi: 10.1111/j.1360-0443.2004.00813.x
33. Samuels J. Personality disorders: epidemiology and public health issues. Int Rev Psychiatr. (2011) 23:223–33. doi: 10.3109/09540261.2011.588200
34. Verheul R. Co-morbidity of personality disorders in individuals with substance use disorders. Euro Psychiatr. (2001) 16:274–82. doi: 10.1016/S0924-9338(01)00578-8
35. Hiebler-Ragger M, Unterrainer HF, Rinner A, Kapfhammer HP. Insecure attachment styles and increased borderline personality organization in substance use disorders. Psychopathology. (2016) 49:341–4. doi: 10.1159/000448177
36. Kienast T, Stoffers J, Bermpohl F, Lieb K. Borderline personality disorder and comorbid addiction. Deutsches Ärzteblatt Int. (2014) 111:280–6. doi: 10.3238/arztebl.2014.0280
37. Samuel DB, LaPaglia DM, Maccarelli LM, Moore BA, Ball SA. Personality disorders and retention in a therapeutic community for substance dependence. Am J Addict. (2011) 20:555–62. doi: 10.1111/j.1521-0391.2011.00174.x
38. Barnicot K, Katsakou C, Bhatti N, Savill M, Fearns N, Priebe S. Factors predicting the outcome of psychotherapy for borderline personality disorder: a systematic review. Clin Psychol Rev. (2012) 32:400–12. doi: 10.1016/j.cpr.2012.04.004
39. Bender DS. The therapeutic alliance in the treatment of personality disorders. J Psychiatr Pract. (2005) 11:73–87. doi: 10.1097/00131746-200503000-00002
40. Olesek KL, Outcalt J, Dimaggio G, Popolo R, George S, Lysaker PH. Cluster b personality disorder traits as a predictor of therapeutic alliance over time in residential treatment for substance use disorders. J Nerv Ment Dis. (2016) 204:736–40. doi: 10.1097/NMD.0000000000000553
41. Wittchen HU, Hoyer J. Klinische Psychologie & Psychotherapie. Berlin Heidelberg: Springer (2011).
42. DiClemente C, Prochaska J. Self-Change and therapy change of smoking behavior: a comparison of processes of change in cessation and maintenance. Addict Behav. (1982) 7:133–42. doi: 10.1016/0306-4603(82)90038-7
43. Prochaska JO. DiClemente, CC, Norcross JC. In search of how people change: applications to addictive behaviors. Am Psychol. (1992) 47:1102–14. doi: 10.1037/0003-066X.47.9.1102
44. De Leon G, Melnick G, Kressel D. Motivation and readiness for therapeutic community treatment among cocaine and other drug abusers. Am J Drug Alcohol Abuse. (1997) 23:169–89. doi: 10.3109/00952999709040940
45. Prochaska JO, Norcross JC. Stages of change. Psychotherapy. (2001) 38:443–8. doi: 10.1037/0033-3204.38.4.443
46. Emmerling ME. Whelton, WJ. Stages of change and the working alliance in psychotherapy. Psychotherapy Res. (2009) 19:687–98. doi: 10.1080/10503300902933170
47. Rochlen AB, Rude SS, Barón A. The relationship of client stages of change to working alliance and outcome in short-term counseling. J Coll Counsel. (2005) 8:52–64. doi: 10.1002/j.2161-1882.2005.tb00072.x
48. Ilgen MA, McKellar J, Moos R, Finney JW. Therapeutic alliance and the relationship between motivation and treatment outcomes in patients with alcohol use disorder. J Subst Abuse Treat. (2006) 31:157–62. doi: 10.1016/j.jsat.2006.04.001
49. Grant BF, Stinson FS, Dawson DA, Chou SP, Dufour MC, Compton W, et al. Prevalence and co-occurrence of substance use disorders and independent mood and anxiety disorders. Alcohol Res Health. (2006) 29:107–20. doi: 10.1001/archpsyc.61.8.807
50. Kessler RC. The epidemiology of dual diagnosis. Biol Psychiatry. (2004) 56:730–7. doi: 10.1016/j.biopsych.2004.06.034
51. World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders Diagnostic Criteria for Research. Geneva: World Health Organization (1993).
52. Derogatis LR, Melisaratos N. The brief symptom inventory: An introductory report. Psychol Med. (1983) 13:595–605. doi: 10.1017/S0033291700048017
53. Franke GH, Ankerhold A, Haase M, Jäger S, Tögel C, Ulrich C, et al. Der Einsatz des Brief Symptom Inventory 18 (BSI-18) bei Psychotherapiepatienten. Psychother Psych Med. (2011) 61:82–6. doi: 10.1055/s-0030-1270518
54. Collins NL, Read SJ. Adult attachment, working models, and relationship quality in dating couples. J Pers Soc Psychol. (1990) 58:644–63. doi: 10.1037/0022-3514.58.4.644
55. Schmidt S, Strauß B, Höger D, Brähler E. Die Adult Attachment Scale (AAS): Teststatistische Prüfung und Normierung der deutschen Version. Psychother Psych Med. (2004) 54:375–82. doi: 10.1055/s-2003-815000
57. Zimmermann J, Benecke C, Hörz S, Rentrop M, Peham D, Bock A, et al. Validierung einer deutschsprachigen 16-Item-Version des Inventars der Persönlichkeitsorganisation (IPO-16). Diagnostica. (2013) 59:3–16. doi: 10.1026/0012-1924/a000076
58. Kernberg OF. Severe Personality Disorders: Psychotherapeutic Strategies. Yale: Yale University Press. (1993).
59. Hasler G, Klaghofer R, Buddeberg C. Der Fragebogen zur Erfassung der Veränderungsbereitschaft (FEVER): Testung der deutschen Version der University of Rhode Island Change Assessment Scale (URICA). Psychother Psych Med. (2003) 53:406–11. doi: 10.1055/s-2003-42172
60. McConnaughy EA, Prochaska J, Velicer W. Stages of change in psychotherapy: measurement and sample profiles. Psychotherapy. (1983) 20:368–75. doi: 10.1037/h0090198
61. Wilmers F, Munder T, Leonhart R, Herzog T, Plassmann R, Barth J, et al. Die deutschsprachige Version des Working Alliance Inventory-Short revised (WAI-SR): Ein schulenübergreifendes, ökonomisches und empirisch validiertes Instrument zur Erfassung der therapeutischen Allianz. Klinische Diagnostik & Eval. (2008) 1:343–58. doi: 10.1002/cpp.658
62. Horvath AO, Greenberg LS. Development and validation of the working alliance inventory. J Couns Psychol. (1989) 36:223–33. doi: 10.1037/0022-0167.36.2.223
63. Hiebler-Ragger M, Perchtold-Stefan CM, Unterrainer HF, Fuchshuber J, Koschutnig K, Nausner L, et al. Lower cognitive reappraisal capacity is related to impairments in attachment and personality structure in poly-drug use: an fMRI study. Brain Imag Behav. (2020) 15:2187–98. doi: 10.1007/s11682-020-00414-3
64. Khantzian EJ. Addiction as a self-regulation disorder and the role of self-medication. Addiction. (2013) 108:668–9. doi: 10.1111/add.12004
65. Fitzpatrick MR, Irannejad S. Adolescent readiness for change and the working alliance in counseling. J Counsel Develop. (2008) 86:438–45. doi: 10.1002/j.1556-6678.2008.tb00532.x
66. Falkenström F, Granstrom F, Holmqvist R. Therapeutic alliance predicts symptomatic improvement session by session. J Couns Psychol. (2013) 60:317–28. doi: 10.1037/a0032258
67. Bachelor A. Clients' and therapists' views of the therapeutic alliance: Similarities, differences and relationship to therapy outcome. Clin Psychol Psychother. (2013) 20:118–35. doi: 10.1002/cpp.792
Keywords: substance use disorder, therapeutic alliance, working alliance dimensions, therapeutic community, attachment
Citation: Rübig LL, Fuchshuber J, Köldorfer P, Rinner A, Fink A and Unterrainer H-F (2021) Attachment and Therapeutic Alliance in Substance Use Disorders: Initial Findings for Treatment in the Therapeutic Community. Front. Psychiatry 12:730876. doi: 10.3389/fpsyt.2021.730876
Received: 25 June 2021; Accepted: 20 October 2021;
Published: 10 November 2021.
Edited by:
Elias Aboujaoude, Stanford University, United StatesReviewed by:
Martin Zack, Centre for Addiction and Mental Health (CAMH), CanadaDeena Marie Walker, Oregon Health and Science University, United States
Copyright © 2021 Rübig, Fuchshuber, Köldorfer, Rinner, Fink and Unterrainer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Human-Friedrich Unterrainer, aHVtYW4udW50ZXJyYWluZXJAdW5pdmllLmFjLmF0